The Skinny on Our Skin
The largest organ in our body is our skin. Weighing on average six pounds, it provides a myriad of critical functions and is involved in a wide variety of jobs that affect the entire body.
As our body’s outer covering, the skin is protective, shielding us from cold, heat, sunlight, infections, and injury. Yet, more than simply a protective covering, it acts as a barrier, protecting our internal organs from environmental toxins and invading organisms.
Our skin also regulates our body temperature as it orchestrates the process of perspiration, and is involved in the elimination of wastes from the body. On the other hand, it is also important for absorption, as it retains water and ushers essential nutrients and molecules back into the body.
Some medications and hormones are absorbed through the skin, then circulate throughout the body and our internal organs. Finally, skin plays a crucial role in absorbing UV light from the sun, and then converting sunlight into vitamin D, an essential element for good health.
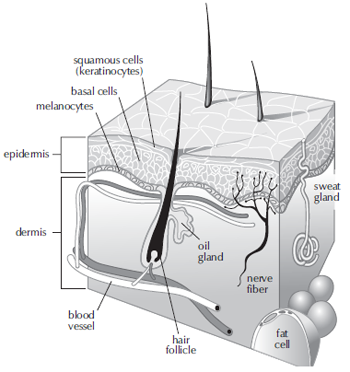 With so many jobs to do, the skin is understandably a complex structure (see figure). It is made up of two layers: the outer layer, or epidermis, and the inner layer, or dermis. The epidermis is thinner than the dermis and contains several different types of skin cells. The majority of cells in the epidermis are squamous cells (flat, scalelike cells also called keratinocytes) that form the most exterior layer.
With so many jobs to do, the skin is understandably a complex structure (see figure). It is made up of two layers: the outer layer, or epidermis, and the inner layer, or dermis. The epidermis is thinner than the dermis and contains several different types of skin cells. The majority of cells in the epidermis are squamous cells (flat, scalelike cells also called keratinocytes) that form the most exterior layer.
Just below the squamous cells are round basal cells, which constantly divide and rise to the outer surface of our skin where they die and then slough off. Interspersed between the basal cells are specialized cells called melanocytes whose main role is to produce a molecule called melanin, or pigment, which gives the skin its color. Melanin is also important as it absorbs UV radiation from the sun and protects the skin from too much sun exposure.
The inner dermis contains a variety of structures including blood vessels, hair follicles, nerve fibers, lymph ducts and glands. These glands produce sweat, which helps to regulate body temperature, as well as sebum, an oily substance that keeps the skin from drying out. Both sweat and sebum reach the skin’s surface through openings called pores.
The dermis also contains two types of fibrous proteins: collagen, the most abundant protein in the skin, and elastin. Collagen provides rigidity and support to our skin while elastin, with its ability to coil and recoil like a spring, gives the skin its elasticity.
Over time, aging and environmental factors contribute to our body’s diminished ability to produce collagen and elastin, causing the skin to wrinkle and sag.
In Hormone Replacement Therapy and the Skin, Dr. Allesandra Graziottin describes the skin as our “multisensory identity card.” She writes, “The skin maintains life-long the written and visible memory of our life. Its characteristics and texture reveal our age and life-styles—particularly related to sun exposure and skincare, but also to the quality of nutrients and stress levels— and the quality of our health.”
Indeed, simply by looking at a person’s skin, we may be able to learn quite a bit about who that person is. Certain features such as wrinkles and scars, and their appearance as well as the location on the body, often reflect the personality of the individual beneath the skin. Our skin is unique to us because it typically mirrors what happens inside our body over the course of our lifetime.
The Skin and Hormones
The skin is where much of the body’s hormonal activity takes place and, according to research studies, then it cannot function without hormones. As a target organ of numerous sex hormones (such as the estrogens, progesterone, and testosterone), the skin contains different types of hormone receptors, including estrogen receptors, as well as receptors for progesterone and testosterone. The anti-stress hormone DHEA and the sleep hormone melatonin are also both found in human skin and are converted to biological molecules with important functions. DHEA is converted into estrogen and other hormone-related molecules found only in the skin. Melatonin is synthesized in the skin and, in low concentrations, is believed to stimulate cell growth. Moreover, hormones produced elsewhere in the body are known to play a role in the health of our skin.
Estrogens
Our skin is one of the central organs known to benefit from higher circulating levels of the estrogen hormones (i.e., estriol, estradiol, and estrone). Receptors for the estrogen hormones are located in both the epidermal and dermal layers, as well as in the blood vessels of the skin. In women, the highest number of estrogen receptors are found in the vagina.
Just as estrogens have beneficial effects in maintaining bone density, high levels of circulating estrogens improve fluid retention, and elasticity in our skin. They also stimulate collagen production and increase the moisture naturally maintained by our skin. There is a strong connection between the amount of collagen in our skin and skin thickness, thus skin thickness may correlate with levels of the estrogen hormones.
With the growing volume of literature on estrogen hormones, it is not surprising to find that some controversy still exists regarding the effects of estrogens on the aging of the skin. In Nutrition for Women, Dr. Ray Peat points out that when treating the skin with supplemental estrogens, water and fat may accumulate in the skin, which is what gives it the appearance of smoothing out wrinkles. He notes that testosterone and progesterone may offer more support by stimulating the production of collagen in the skin.
Testosterone
Our skin is also sensitive to the action of testosterone. In fact, one of the ways in which testosterone is excreted is through glands within the layers of the skin as sebum. Teenagers experiencing surges of testosterone during puberty typically develop acne from blocked skin pores that become clogged with surplus sebum. Because testosterone levels naturally decline as we grow older, an insufficient amount of oil may be produced, and this often causes the skin— particularly on the face and hands—to become noticeably dry. Decreases in testosterone may also result in thinning of the skin as collagen production declines.
Thyroid
Thyroid contributes to overall skin health. In general, normal levels of thyroid hormone are associated with better hydrated skin, as well as with thicker, healthier-looking skin. Now that there are medical tools that measure the circulation of blood throughout our skin, we have a better understanding of the importance of thyroid hormone in maintaining healthy skin.
Studies show that a low functioning thyroid may result in reduced blood circulation. In advanced cases of hypothyroidism (when the body produces too little thyroid hormone), the skin may receive as little as 20 to 25 percent of the normal blood supply. With reduced circulation, the nourishment supplied by blood is compromised and waste products are not removed promptly and completely.
Hypothyroidism may result in skin that becomes less resistant to potential infection. Our skin plays host to a wide range of bacteria, some of which are quite damaging if they are able to gain access through the skin, invade, and then multiply. When thyroid function is compromised, so is the skin’s ability to act as a barrier, and the body becomes more prone to infections.
Possible Deficiency |
Skin-Related Symptoms |
| Estrogen | Tiny vertical wrinkles around lips; dry, thin, and/or pale skin; little wrinkles around eyes; smile lines |
| Testosterone | Lots of wrinkles; small wrinkles around eyes or mouth; creased forehead; dry, thin, and/or pale skin; sun sensitivity; slow to heal |
| Thyroid | Dry and/or pale skin, skin cancer |
| Melatonin | Age spots, skin cancer |
| Growth Hormone | Lots of wrinkles, large wrinkles on sides of nose and mouth, small wrinkles around eyes or mouth, creased forehead, dry and/or thin skin, slow healing |
| DHEA | Age spots, dry skin |
| Some related symptoms may be associated with a hormone deficiency. (Adapted from The Hormone Solution by Dr. Thierry Hertoghe) | |
Reduced circulation of blood through the skin is just one effect of low thyroid function. Other related effects include an unhealthy appearance due to thinning, dryness, and loss of color. Yet another potential symptom of low thyroid function is overproduction of a gel-like substance in the skin called mucin. Because mucin has a high affinity for water, it can attract and hold excess water, leading to swelling all over the body.
Human Growth Hormone
Human growth hormone (HGH) also plays a role in the health and vitality of skin. In middle and late adulthood, we all tend to experience a number of changes in body composition, including shrinking of lean body mass, expansion of fat tissue, and thinning of the skin. In a landmark study published in 1990, Dr. Daniel Rudman and colleagues reported that adding back HGH could actually reverse the effect of thinning skin. The results of their study showed that skin thickness increased more than 7% among men who received HGH for six months, whereas no significant changes in thickness occurred in a group receiving no treatment. This was the first study to demonstrate that a diminished growth hormone level is responsible, at least in part, for the thinning of skin that occurs in old age.
Canvas for Hot Flashes
A discussion about skin and the role of hormones is not complete without a mention of hot flashes. Hot flashes and their accompanying sensations of sweating are acknowledged by many women and their clinicians as some of the most common symptoms of menopause. This is certainly the case with Caucasian women, although worldwide and within different cultures, there is considerable variation in the prevalence of these symptoms.
Triggers, Symptoms, and Frequency
Hot flashes may occur at any time of the day and night, and they are triggered by a variety of actions as mundane as sleeping, working, relaxing, eating spicy food, and drinking tea, coffee, or alcohol,. The symptoms accompanying a trigger are also varied, but the most common may include a feeling of increased pressure in the head. During the night, a decrease of rapid eye movement (REM) sleep and waking often precede a hot flash. For most women, hot flashes arise as a sudden feeling of heat in the face, neck, or chest, and they are often associated with patchy flushing of the skin and profuse perspiration. The initial focal point may be very specific, such as an ear lobe, the forehead, or the area between the breasts, but a subsequent spread of the heat sensation may continue upwards and downwards throughout the body. Heart palpitations also frequently accompany a hot flash. When these episodes occur at night, a “domino effect” then often leads to insomnia, irritability, and general lethargy.
The frequency of hot flashes varies among individuals, ranging from a few per month to several per hour; up to fifty per day have been reported. Similarly, the duration of a hot flash may range from a few seconds up to one hour, although the average duration is usually around three minutes. In most women, hot flashes and their associated symptoms may persist for over a year, and approximately 25% of women who experience hot flashes report that they persist for more than five years.
The Physiology of Hot Flashes
The physiologic changes that accompany hot flashes include a sudden increase of blood flow to the skin, which then warms the skin and provides the sensation of a sudden rise in temperature. A medical device that measures body temperature changes shows that during the course of a hot flash, such alterations occur over most parts of the head, neck, trunk, and limbs. Although the greatest temperature changes are found in the fingers and toes, hot flashes are usually felt most strongly in the face, neck, and upper trunk. Research indicates that the sensation of heat is often out of proportion to the actual temperature increase measured during hot flashes. Furthermore, the temperature increase often persists for several minutes after the sensation of warmth has passed, indicating that women experience a hot flash only while their skin temperature is increasing. The severity of the sensation is therefore probably related more to the rate of temperature change than to the actual temperature increase.
Hot Flashes and Hormones
The clinical value of estrogen therapy in helping to alleviate hot flashes is well established, although the exact mechanism by which this occurs is not yet understood. In some studies, women with severe hot flashes had significantly lower mean body weight and levels of total estrogen and estradiol than women without hot flashes. These findings suggest that body size and its effects on the metabolism of naturally occurring estrogens may be a factor in the occurrence of hot flashes in postmenopausal women.
Women with hot flashes also tend to have more extreme changes in their cycle of estradiol production, suggesting that the rate of change in estrogen levels could be a trigger for hot flashes. This also suggests that each individual may have a specific range of estrogen levels within which hot flashes will occur, once they reach their specific threshold. This variability among individual women points to the value of trying estrogen therapy and working with a trained practitioner to help determine the amounts of estrogen hormones that are most effective in alleviating hot flashes and other uncomfortable symptoms of menopause.
Supplemental progesterone has also been effective in treating hot flashes. A study by Dr. Helene Leonetti established that progesterone cream applied to the skin of menopausal women helped alleviate hot flashes and excessive sweating. As in the case of estrogens, the mechanism by which progesterone controls hot flashes is not well understood.
Cellulite
Hormones, specifically estrogens, are a primary cause of cellulite, and this explains why men, who have much less estrogen than women, never get cellulite. Secondary to hormones in the formation of cellulite is genetics. As many of us have learned, cellulite tends to be hereditary, so if your mother had cellulite, you are more likely to have it as well.
Due to hormones and genetics, blood vessels in the skin tend to weaken and further contribute to the formation of cellulite. The weakening of blood vessels explains why many women tend to develop spider veins and bruise very easily, especially on their thighs. Cellulite becomes visible when areas of the skin become so weakened that they break down and allow fat cells below the skin layers to push their way through the skin and to the surface. The best way to get rid of cellulite and related stretch marks is to work on repairing the damaged dermis, rather than concentrating on burning fat.
Detoxification Pathway
While we mainly think of the skin as a gateway for elements ranging from sunlight to moisturizing lotions, to hormones, it is important to remember that it has another critical function: that of detoxification. When too many toxins overwhelm the liver, intestinal tract, and kidneys, the skin is called into action. This is most apparent when toxins exiting the skin combine with surface bacteria, resulting in blemishes and acne. While acne is most frequently seen in adolescence, many women develop acne during midlife transition when, as in adolescence, the liver can be overwhelmed by sudden bursts of estrogens.
In The Ageless Woman, Dr. Serafino Corsello cautions that “if the liver is not adequately supported by appropriate nutrients, the skin may wear the brand of toxicity.”
Hormone Absorption
Another important relationship between skin and hormones involves the application of hormones directly to the skin as a method of hormone treatment. Sex hormones are well-suited for absorption through the skin. Studies demonstrate that, when applied to the skin, the sex hormone molecules can move through the various layers and then circulate in the blood to other organs of the body.
A variety of factors affect the skin’s ability to absorb hormones, including thickness, hydration (dry versus oily), the size of the application area, where on the body the hormone is applied, the length of exposure, and the type of formulation (such as a cream, gel or patch).
Because everyone’s skin is different, absorption will vary. For example, skin thickness, fat cell content, and skin cell dimensions are different from individual to individual, and this even varies at different locations on the same person. In general, hormone absorption varies from one person to another and is affected by where on the body a hormone is applied. The sites of greatest hormone absorption are the head, neck, scrotum, and armpits.
It is also important to know that other factors affect the skin’s ability to absorb medications and hormones. One study looked at estradiol absorption when applied as a gel to three different-sized areas of the skin in postmenopausal women. The results indicated that absorption was greatest when applied to the smallest area of skin. Moreover, absorption through the skin was affected by washing the application site. Estradiol absorption was significantly reduced at the two smallest application sites when they were washed 30 minutes after the gel was applied. Thus, when applying hormone treatment to the skin, it may be more effective to apply a concentrated amount to a smaller patch of skin and then wait before washing the area.
Hormone Changes and Hormone Therapy
The critical roles that hormones play in maintaining skin health may help explain why hormone changes that accompany aging and menopause have such a deep impact on our skin. These changes involve not only the way in which our skin functions, but its appearance too.
Hormonal changes affect collagen and elastin production, the function of nerve endings, the flow of blood within vessels, and the secretions of glands. As we age and our hormone levels change, the skin tends to become more acidic. Fluctuations in skin secretions may alter the smell of our skin, and changes in hydration, texture, and the relative percentages of collagen and elastin content certainly can affect the look and feel of our skin over time.
Dr. Mark Brincat was one of the first to quantify the decrease in skin collagen after menopause. He found that the decrease in collagen and subsequent decline in skin thickness is what causes a thin and somewhat translucent appearance. However, this may be reversed with adequate estrogen therapy.
Aging results in decreased estrogen activity and enzymes that convert DHEA to estrogen also decline. Women who take estrogens tend to have thicker, healthier skin, and women who take both estrogens and testosterone tend to have skin that is significantly thicker (and healthier) than women who don’t take either hormone.
Hormone therapy may slow the impacts of aging and menopause on the skin’s appearance, in ways that are both direct and indirect. Direct effects include improvements in skin collagen and elastin activity, and increased sweat and sebaceous secretions. Indirectly, hormone therapy leads to improvements in blood vessels, nerve, and immune system functions.
The health of our skin is intimately entwined with our hormones. Therefore, clinicians who specialize in treating and caring for skin may be able to detect particular hormone deficiencies based upon the appearance of the skin and certain symptoms.
Connections is a publication of Women’s International Pharmacy, which is dedicated to the education and management of PMS, menopause, infertility, postpartum depression, and other hormone-related conditions and therapies.
This publication is distributed with the understanding that it does not constitute medical advice for individual problems. Although this material is intended to be accurate, proper medical advice should be sought from a competent healthcare professional.
Publisher: Constance Kindschi Hegerfeld, Executive VP – Women’s International Pharmacy
Co-Editors: Julie Johnson; Carol Petersen, RPh, CNP – Women’s International Pharmacy
Writer: Kathleen McCormick – McCormick Communications
Illustrator: Amelia Janes – Midwest Educational Graphics
Copyright © Women’s International Pharmacy. This newsletter may be printed and photocopied for educational purposes, provided that your copy (or copies) include full copyright and contact information.
 For more information, please visit womensinternational.com or call 800.279.5708.
For more information, please visit womensinternational.com or call 800.279.5708.
Women’s International Pharmacy | Madison, WI 53718 | Youngtown, AZ 85363
